SPACE
Hospitals’ strategies regarding how to use space were often innovative and showed proof of adaptability, which made it possible to handle the challenges of the physical environment. Relocation and repurposing were frequently the answer.
Resilient organisations understand how hospitals can adapt and grow through the current pandemic. The study below aims to share information between professionals for a better future resilience.

The four project partners are Ramboll, Comentum, White arkitekter and the European Health Property Network. Together, they represent expertise in healthcare architecture and engineering, process and system redesign, health policy and healthcare capital asset investment. They collectively have interests in the design of physical and digital healthcare infrastructure, the links between the built environment and the safety, quality and efficiency of clinical processes. They also have expertise in the costs associated with different environment and care models, change management and how to ensure sustainable improvements in healthcare systems.

Ramboll is a leading engineering, architecture and consultancy company founded in Denmark in 1945.
Ramboll employs 16,500 people globally and has especially strong representation in the Nordics, UK, North America, Continental Europe, Middle East and Asia-Pacific. We are present in 35 countries and combine local experience with a global knowledge base, constantly striving to achieve inspiring and exacting solutions that make a genuine difference to our clients, end users and society at large. Ramboll works across the following markets: Buildings, Transport, Water, Environment & Health, Energy and Management Consulting.
You can find out more about Ramboll here.

Stockholm-based Comentum specializes in change and innovation management in healthcare and the life sciences. We work with hospitals and healthcare organizations in Sweden, Norway and Switzerland. We enable organisations to succeed with strategic projects that matter. We help focus on the right things by sustainably integrating innovation throughout. Our clients share our enthusiasm for sustainable initiatives at the intersection of behavioural, process and technological change.
Together with our clients, we co-create change processes that energize and provide focus to achieve impact. We focus on structuring the organizational development in connection with large-scale building projects in healthcare and life science. This includes the set-up of project offices and innovation frameworks. We help you with user involvement - both employees and patients - and with testing the future way of working before the move.
There are great ideas out there that have the potential to make healthcare a better place for patients and those who care for them. Let us capture them! The expertise and experience of healthcare professionals are the biggest assets for transformations in healthcare. Let us catalyse them!
You can find out more about Comentum on www.comentum.co
If you wish to get in touch directly please reach out to Micha Kämpfer (CEO) via micha.kaempfer@comentum.se.

White Arkitekter is one of Scandinavia’s leading architectural practices. We work with sustainable architecture, urban design, landscape architecture and interior design for current and future generations. Our mission is to enable sustainable life through the art of architecture. Our vision is that by 2030 all our architecture will be climate neutral, through design excellence.
We work with sustainable architecture, design and urban development in an international context. We need to act responsibly, as our work affects the lives of many both present and future generations. We create spaces for people to thrive and grow in harmony with the ecosystem that we inhabit. We act responsibly by operating within the sustainable limits of our planet when we design healthy living environments that inspire and engage.
Our curiosity is reflected in the way we work. We believe that the search for new knowledge will strengthen our offer for the future. Therefore, we continuously invest in research and development. Through design, creativity and a humanistic approach, we look to solve great challenges. We believe that architecture is shaped by the unique qualities of its context. This makes us radical contextualists.
We are an employee-owned company, and we value involvement and participation. We respect the equality of every individual, and we believe everyone has the right to a sustainable life. This is the foundation of our architecture and our culture. Our projects evolve in collaboration with our clients, users, partners, colleagues and other stakeholders.
By being good listeners, understanding varying perspectives and being devoted to collaboration, we create lasting value.
You can find out more about White Arkitekter here.

The European Health Property Network (EuHPN) exists to pool the knowledge from its member organisations to promote a better understanding of how to plan, design, build, maintain and finance all kinds of health facilities, from the largest university teaching hospitals to the smallest clinics and primary care centres. Our members represent interests in healthcare architecture, healthcare capital asset investment, health facility design research and health estate development. The network currently has around 20 member organisations from a range of European countries, plus associate individual and organisation members.
You can find out more about the EuHPN here.
The partner organizations, which provided pro bono resources to make the project a reality, and are grateful for additional financing provided by the following institutions:
Ramboll Foundation, Denmark
Forum Vårdbyggnad, Sweden
White Research Lab, Sweden
Jonathan Erskine - European Health Property Network
Bo Rytkjær Callesen, Flemming Schmidt, Katarina Ringstedt, Michael Stevns - Ramboll
Micha Kaempfer, Anne Richter - Comentum
Jetri Regmi - World Health Organization
Andrea Brambilla - Politecnicodi Milano
Christopher Shaw - Architects for Health
Liesbeth van Heel - Erasmus MC
Charlotte Ruben, Christiana Caira, Saga Karlsson - White Arkitekter
Susan Grant & Michael Cassells - NHS
Ana Maria Alvarez - Pinearq
John Avdoulos & Camilla Moretti - HKS
Pilosof Nirit - Cambridge University
Björn Hollström - Region Stockholm
Birgitte Gade Ernst - Arkitema
Eduardo Teran - Estudio 15arquitectos
Amie Shao - Mass design group
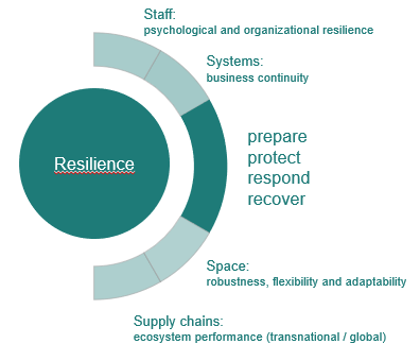
The Relocate, Repurpose, Reorganize project is fundamentally about learning from the hospital experience of the COVID-19 pandemic to provide guidance on how hospitals and health systems can become more resilient. To do this, it focuses on staff, systems, space and supply chains.
From early in the pandemic, resilience became the watchword across global health systems, referring first to the ability of hospitals and public health systems to respond to the first wave of the crisis and later to their capacity to return to normal functioning.
From our desk research, the project team adopted the following working definition of resilience: the capability to maintain and adapt critical functions when faced with changes.
The project uses desk research, regularly updated, to scan emerging literature and intelligence in each of the four focus areas. In addition, it builds a library of case studies to offer insights into the responses of hospitals and health systems in disparate countries and contexts.
Taken together, the desk research references, the case studies and the web-based field guide are a resource for everyone involved in learning how to make hospitals and health systems more resilient to future crises in public health.
As the COVID-19 epidemic unfolded across the world, healthcare systems in general, and acute hospitals in particular, had to make urgent and radical adjustments to the capacity, processes and care models for diagnosing and treating patients. The impact was felt across the system, but especially strongly in departments dealing with emergency, critical and respiratory care.
The response in hospitals encompassed every aspect of the organisation: the physical layout and arrangement of space, how staff should work, the nature of the systems (including IT and communications) that support clinical and non-clinical work and the capability and capacity of supply chains to ensure that equipment, drugs and medical devices were available.
As underlying concepts and assumptions were necessarily uncertain and solutions had to be found at speed, the project partners kick-started learning by taking the opportunity to compare the arrangements found in diverse countries and organisations. A mix of desk and case study research was used to examine all four areas of space, staff, systems and supply chains and to synthesise the lessons learned into a web-based field guide. The overarching aims were to learn from the varied experiences of hospitals and health systems, to make this knowledge available to all and to contribute to building hospital and health system resilience.
The project has four main goals:
The project partners conducted rapid desk research in March and April 2020 to examine the hospital sector’s response to the first wave of the pandemic.
In relation to hospital infrastructure, this revealed common patterns across many countries:
In addition to changes to the built environment, the partners also noted that staffing, systems and supply chains were areas of major disruption and change. Based on these early observations, the partners agreed to conduct further desk research and to seek a broad range of real-world case studies. The desk research used purposive sampling of the rapidly emerging academic and practitioner literature, with contributions from all the partner organisations. The case studies, which mainly focused on Europe and North America, were chosen for the insights they could provide in relation to the ‘4Ss’ – staff, systems, space, supply chains—within the overall context of hospital and health system resilience. The case studies reflect a range of health system types and encompass acute and teaching hospitals of different sizes and organisation types.
Many of the case studies were presented and discussed at four international webinars. The outputs’ combination of case studies and desk research formed the basis of this web-based field guide, with four main goals:
The field guide is an open access resource, intended to help hospital organisations, policy makers, health system planners, architects, engineers and clinicians make choices about how to organise space, staff, systems and supply chains to meet the ongoing challenge of the COVID-19 pandemic and future public health crises. It is a framework for enquiry and discussion, not a set of definitive answers.